About the procedure
What is a pilonidal sinus?
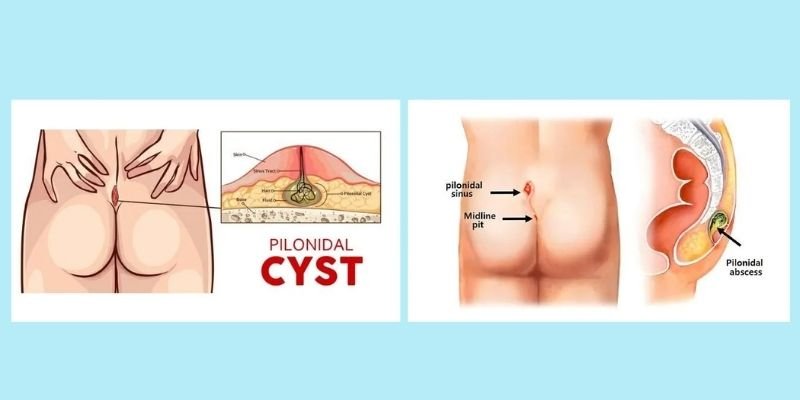
A pilonidal sinus (also called pilonidal cyst or pilonidal disease) is a small tunnel or hole in the skin in the crease between the buttocks (the sacrococcygeal region), typically containing hair, skin debris and bacteria. "Pilonidal" means "nest of hair." The condition is caused by in-grown hairs that penetrate the skin, trigger an inflammatory reaction, and create a sinus tract lined with granulation tissue.
Pilonidal disease ranges from an asymptomatic pit to a large infected abscess or chronic discharging sinus. Acute pilonidal abscess causes severe pain and swelling that requires emergency drainage. Chronic pilonidal sinus causes persistent or intermittent discharge, swelling and discomfort that prevents comfortable sitting or driving.
Surgery is the definitive treatment. The appropriate technique depends on whether the disease is acute (incision and drainage of abscess) or chronic (complete excision of the sinus and tracks, with primary closure or healing by secondary intention). Laser treatment of pit tracts is also available for selected cases of minimal disease.