About the procedure
Laparoscopic ventral hernia repair
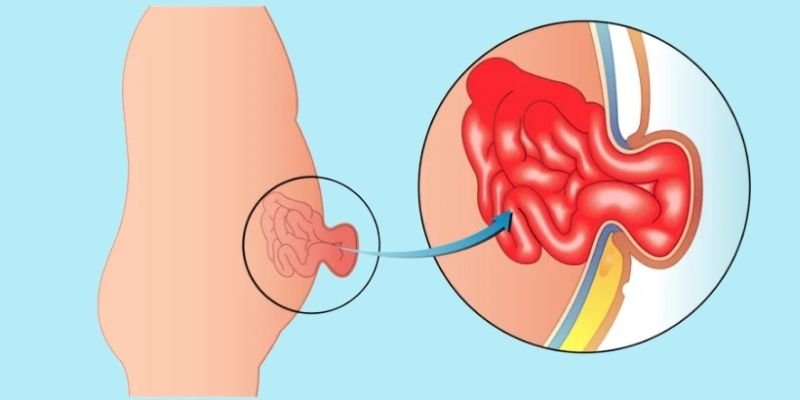
A ventral hernia is a condition where tissue or part of the intestine pushes through a weak spot in the abdominal wall, creating a visible bulge. Many patients experience discomfort, pain, or cosmetic concerns — especially after previous abdominal surgeries, where scar tissue is inherently weaker than normal abdominal wall. While some hernias may appear small and harmless at first, they can gradually enlarge and lead to serious complications if left untreated.
Traditionally, ventral hernias were repaired with open surgery involving large incisions, longer hospital stays, and extended recovery times. Today, laparoscopic ventral hernia repair using the IPOM (Intraperitoneal Onlay Mesh) technique is the preferred approach for most patients. The mesh is placed inside the abdominal cavity through keyhole incisions — completely avoiding any dissection through the existing scar. This produces significantly less pain, faster recovery, and a dramatically lower wound complication rate compared to open repair.
At our practice, we combine over 25 years of surgical expertise, 8,000+ successful laparoscopic surgeries, and advanced technology to deliver world-class hernia repair with a patient-first approach.
Types of ventral hernia
A ventral hernia refers to any hernia through the front abdominal wall. Common types include:
Incisional Hernia
Develops at the site of a previous surgical scar — the most common type, occurring in approximately 10–15% of all abdominal operations. Typically appears 1–3 years after surgery.
Umbilical Hernia
Occurs at or near the navel (belly button). Common in adults with obesity, multiple pregnancies, or conditions that cause persistent abdominal straining.
Epigastric Hernia
Appears between the belly button and the lower chest. Often small but can cause persistent discomfort, especially on bending forward or coughing.
Spigelian Hernia
Occurs along the side of the abdominal wall at the semilunar line. Less common but sometimes missed because the bulge is not always visible externally.
All types occur when abdominal muscles weaken, allowing internal tissues to protrude. All require surgical repair — hernias do not resolve on their own.