Understanding the condition
GERD, hiatus hernia & laparoscopic anti-reflux surgery
Gastroesophageal reflux disease (GERD) is one of the most common digestive problems affecting people today. Many patients experience persistent heartburn, regurgitation, chest discomfort, or difficulty swallowing that does not improve with lifestyle changes or medications. Over time, untreated GERD can significantly affect quality of life, disrupt sleep, and lead to complications such as oesophagitis, Barrett's oesophagus, or strictures.
For patients who continue to suffer despite medication, laparoscopic anti-reflux surgery (Nissen fundoplication) offers a permanent, long-term solution. Using minimally invasive techniques, the surgery restores the natural barrier between the stomach and oesophagus — reducing reflux and providing lasting relief that medications cannot achieve.
At Sterling Hospitals, Vadodara, we combine over 25 years of surgical expertise, modern laparoscopic technology, and a patient-first philosophy to deliver safe, effective, and compassionate care.
What is laparoscopic GERD surgery?
Normally, a muscular valve called the lower oesophageal sphincter (LES) prevents stomach acid from flowing backward into the oesophagus. In GERD, this valve becomes weak or relaxed — allowing acid and stomach contents to reflux upward. A hiatus hernia (where part of the stomach herniates through the diaphragm into the chest) further weakens this barrier.
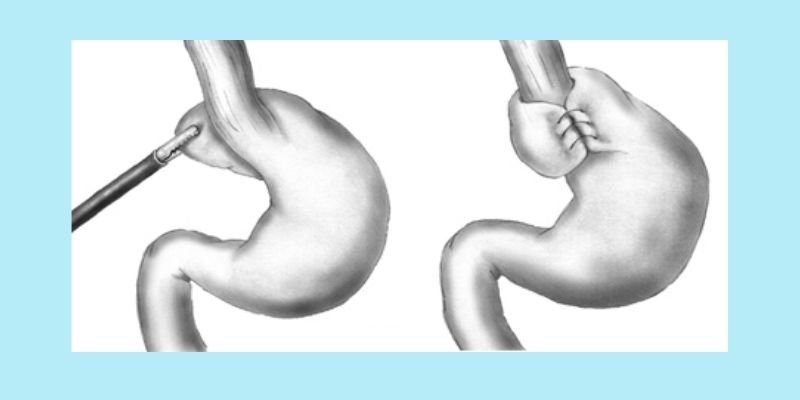
Laparoscopic GERD surgery corrects both problems simultaneously. The hiatal hernia is repaired and the gastric fundus (upper stomach) is wrapped around the lower oesophagus to recreate a competent valve — a fundoplication. The laparoscopic approach uses 5 small incisions and is performed entirely through keyhole instruments.