About the procedure
What is an anal fistula?
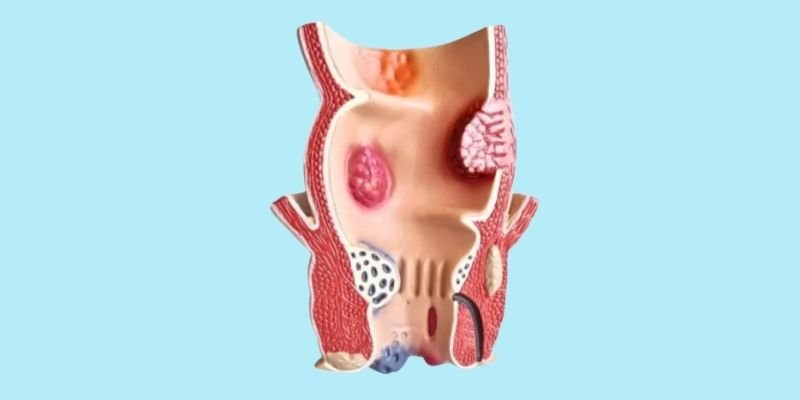
An anal fistula is an abnormal tunnel (tract) connecting the inside of the anal canal to the skin surface around the anus. Most anal fistulas develop after an anorectal abscess — the abscess bursts or is surgically drained, but a residual tract persists, discharging pus, blood or mucus intermittently onto the skin. This causes persistent wetness, soiling, itching and discomfort around the anus.
Fistulas are classified by their relationship to the anal sphincter muscles: intersphincteric fistulas (most common — pass between the sphincter layers), trans-sphincteric fistulas (cross both sphincters), and suprasphincteric or extrasphincteric fistulas (complex, rare). The classification determines the surgical approach, as the sphincter muscles that control continence must be carefully identified and preserved.
The treatment for anal fistula is always surgical — fistulas do not heal with antibiotics alone. Simple fistulas are treated with fistulectomy or fistulotomy. Complex fistulas (involving significant sphincter muscle) are treated with sphincter-preserving procedures such as the LIFT technique.